The experiences and results from the measurements at the Kungälv Hospital provided valuable knowledge for the final field study in DR Congo, including more insights on where to place the air cleaners (height, distance from each other, etc.) and the required air cleaning capacity. We also learned about the impact of clothing and protective equipment on airborne bacteria and particles.
The results from Kungälv also gave us reason to slightly renew the design of the air cleaners. The Swedish manufacturer Light Air therefore developed yet another prototype. The same technology with electrostatic filtration as before, but higher capacity with a straight rectangular filter for easier washing.
Two hospitals were identified already in the project description for installation and testing, both in Bukavo, South Kivu, which borders Rwanda to the east. One is the Panzi Hospital (Figure 1), with about 450 employees, known for the work of Nobel Peace Prize winner Dr Denis Mukwege to help women affected by sexual violence; the other is a smaller hospital, CELPA Hospital, in the city centre (Figure 2) with just over 60 employees. A total of three weeks were spent on site in Bukavu


Results
The measurements in Congo gave good results. The installations had a significant impact on the amount of airborne bacteria. High air purity was achieved despite very tough conditions. They also showed that clothing and protective equipment had a clear impact even in the tested conditions.
The results were particularly good at the CELPA hospital, where the air cleaners could be installed as intended. In their operation room, the bacterial content was reduced by an average of 96%, from 1,700 to 60 CFU/m3 (bacterial colony forming units) during real surgery with six air cleaners, although the capacity of the air cleaners was reduced by about 20% due to low voltage in the hospital area (about 200 V instead of 230 V). The obtained bacterial content is in line with Swedish guidelines1 of a maximum of 100 CFU/m3 in general surgery and 10 CFU/m3 in surgery that is particularly susceptible to infection (Table 1).
Table 1: Results from the CELPA Hospital – real operations.

The study was also able to quantify the impact of clothing and “boots”, which was most clear in the simulated operations, with controlled conditions where these aspects could be isolated (Figure 3).
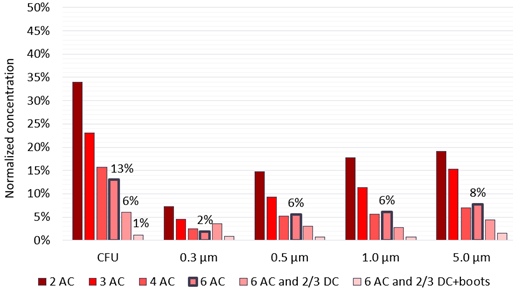
“AC” = air cleaner. “2/3 DC” = two of three wearing disposable clothes. “boots” = plastic bags over shoes up to the knee.
Installations
Although the hospitals had multiple operation rooms, the intention throughout the process was to install the concept in one operation room in each hospital.
In October 2024, the following equipment was shipped by air freight to Bukavu in DR Congo:
- Twelve air cleaners (Light Air)
- Two supply air fans with associated duct parts, filters, etc.
- Two dehumidifiers (Woods)
- Disposal clothes (Mölnlycke Health Care)
In November, the materials arrived in Bukavu, after which the installation work could begin.
Temporary installation at Panzi Hospital
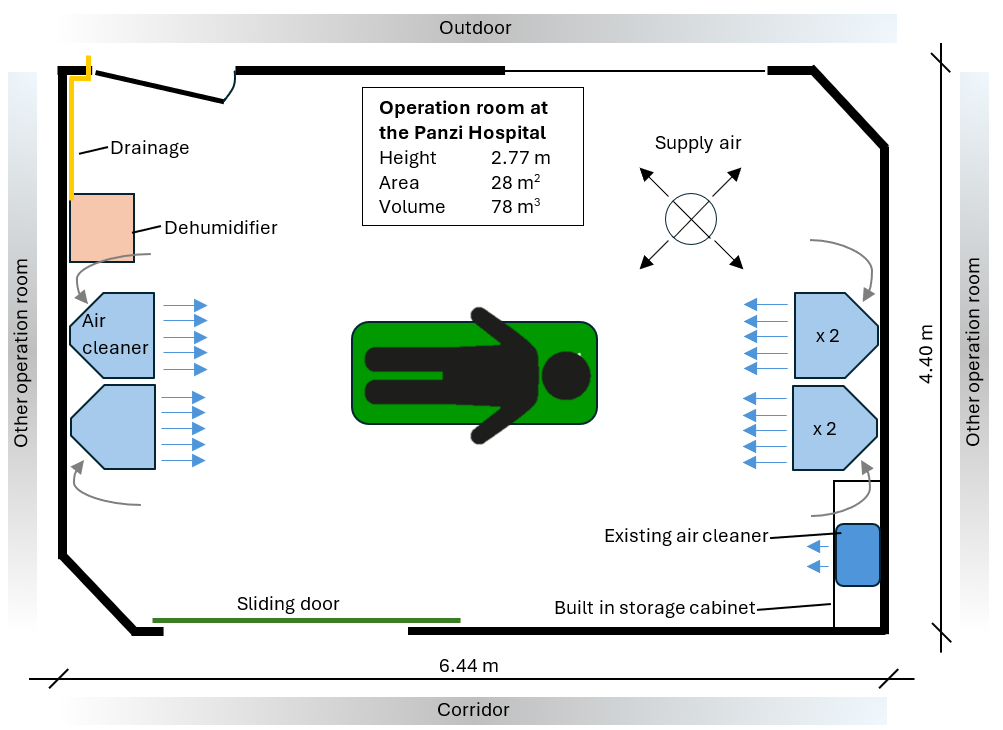
As the intended location turned out to be under construction, we had to carry out a temporary installation in a modern adjacent surgery block named AMISI (African Institute for Minimally Invasive Surgery). The AMISI building houses several operation rooms. We were assigned a room that is mostly used for urological and gynecological surgery, with modern surgical equipment and modern surfaces of sheet metal and glass, see Figure 4. The room also had mechanical supply air, but it was set to very low flow. The exhaust air was turned off. There was also a small air cleaner, which was also set to very low flows. Dilution measurements showed that the ventilation system only delivered a clean air flow rate (CADR) of about 30 l/s and the air cleaner about 36 l/s.

For space reasons and to avoid damage to walls and ceilings, the air cleaners were stacked on the floor on opposite sides of the room. See Figure 5 – 7. The dehumidifier was also placed on the floor, which required drilling a hole through a door frame to drain the condensation water via a hose. The chosen placement was the only one possible, given the conditions.


The operation rooms in the AMISI building have large sliding doors with sensors for automatic opening and closing. However, the doors do not close tightly against the floor and walls, which means that the ventilation system’s low airflows failed to create a measurable overpressure towards the corridor or outdoors.
Once the construction work at the Panzi Hospital is completed, the temporarily installed equipment in the AMISI building will be moved and permanently installed in one of the operation rooms in the new bloc. However, since the new premises will lack ventilation, a supply air unit will also be installed (the same design as at the CELPA Hospital; see below).
Permanent installation at the CELPA hospital
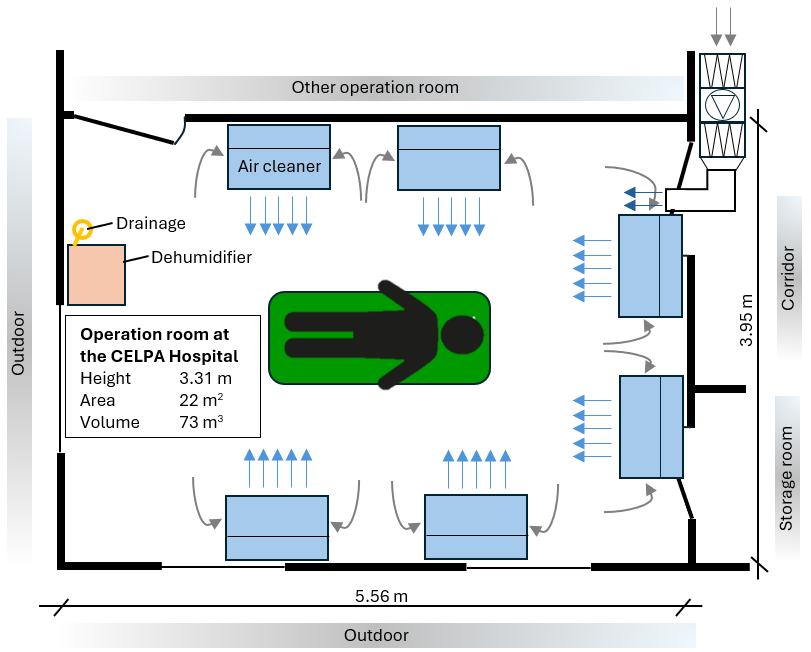
Compared to the Panzi hospital, the CELPA hospital is more representative in an African context regarding building materials, equipment, etc. There are two operation rooms in a single bloc, one mainly used for orthopaedics and the other for other surgery with many caesarean sections. Since orthopaedics is susceptible to infection, the installation was made there. The room is slightly smaller than the one at Panzi but was perceived as more spacious because there was less furniture and other equipment.
The operation room had no mechanical ventilation. There were four mosquito-netted air holes just under the false ceiling, but these were immediately sealed with wooden boards at the request of the hospital management.
The six air cleaners were hung on three of the room’s walls, close to the ceiling and angled down towards the patient (Figures 8 and 10). In the corridor outside the operation room, a supply air unit was installed with a coarse filter (filter class: G4), a fine filter (filter class: F7) and a fan (Figures 9 and 10) and some ducts. A door was always open to the courtyard in the corridor, about four meters from the ventilation unit.
Initially, a fan flow of 80 l/s was intended, giving the room some overpressure (1.5 Pa). But the fan stopped several times for unknown reasons, possibly due to the varying and low voltage in the area. When the airflow was reduced to 20 l/s, the problem ceased. The overpressure in the room then dropped to almost zero.


Method
The impact of air cleaners and clothing could be quantified by measuring the air’s particle and bacterial content. Bacteria were measured with an active biological sampler (Klotz Impaktor, FH6), and the particle content was measured with a particle counter (TSI AeroTrak, 9303). The measuring instruments were always placed as close to the surgical wound as possible, which meant 50 – 70 cm in practice (see Figures 11 and 12). The measurement observers kept their distance from the surgical wound.
In addition to measurements during real surgery, measurement studies were also carried out during simulated surgery under controlled and limited conditions regarding:
- number of people and placement (always two people at the operation table and one person in the corner of the room)
- door openings (always locked)
- clothing (see Figures 13 and 14)
- physical activity
The latter was ensured through a proprietary and time-limited test cycle with predetermined and surgically similar movement patterns.
In both real and simulated operations, the initial measurements were carried out under original conditions to create a baseline. At the Panzi hospital, their regular ventilation was active, as was their existing air cleaner. It also meant that all staff wore 100% cotton clothing. The corresponding situation at the CELPA hospital meant no ventilation, but the clothing for observers and assistants was more modern and made of synthetics (65% polyester and 35% viscose), although extensively washed. However, the surgeon and his assistant mostly wore cotton clothing at the CELPA. Once the baseline had been established, measurements followed where the new installations were activated. The impact of disposable clothing for the staff closest to the patient was also investigated with measurements.



Collaboration with hospital staff
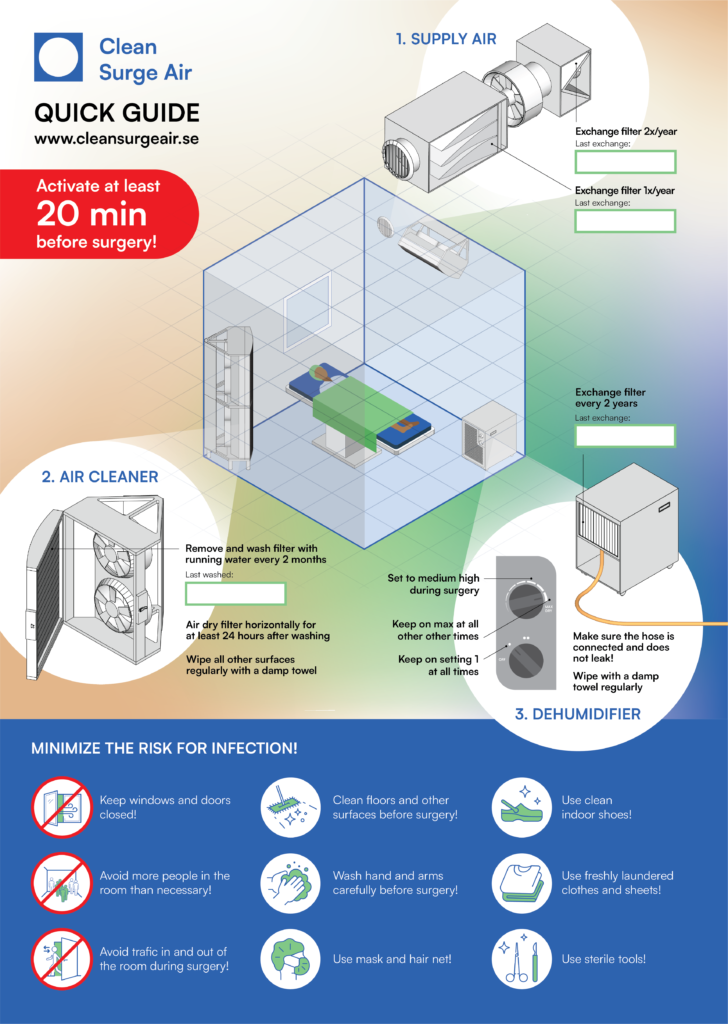
The staff were very cooperative, and many wanted to know more about the project. We, therefore, had briefings with several of the staff members, and we explained the background, purpose, method, technology, and the concept as a whole. We also showed them how the air cleaners filters are washed with water and how ventilation and dehumidifier filters are changed. During the discussions, we used information material on an A3-format plastic sheet that explains the concept and its context, etc. (Figure 15). It also shows how often filters should be washed/changed. Dates are noted in the white fields. The illustrations were produced by the Swedish design agency BOID and were hung visibly on site.
Technical staff at the Panzi Hospital were instructed on how to carry out the permanent installation. They also visited the CELPA Hospital to study the installation there.
Finally, staff and managers at both hospitals expressed great gratitude, and we received several requests for further installations in other operation rooms.
Discussion
Clinical studies from several decades during the 20th-century point to poor air quality in operation rooms as a risk factor for postoperative infections2 (surgical site infections – SSI). Operation rooms in hospitals with financial and technical means are therefore equipped with extensive ventilation devices, which provide them with clean air, but at a high economic and technical cost.
In low-income countries, such technical arrangements are not possible. At the same time, earlier studies, e.g. Lancet3 , show that the SSI-frequency is high in low-income countries. Local conditions, such as air quality and clothing, are probably important factors in this context.
This study in two hospitals in the DR Congo has shown that simple air cleaners significantly reduce airborne particles and bacteria (especially in combination with appropriate clothing), which can positively impact SSI. Follow-up prospective clinical studies in this regard would be very interesting.
Acknowlegdement
We want to express our sincere gratitude to all those who were helpful during our stay in DR Congo. At the risk of missing some, we would like to extend a special thank you to the medical staff at Panzi Hospital and CELPA Hospital, represented in this context by M. Asher Ngabo, Dr. Aline Kusinza, Dr Sosthene Birhange, and M. Badarhi Bahati. Finally, we would also like to mention M. Ben Pletincx (BST Medical BV) and Dr Angélique Neema Ciza (MGP System) for all their help related to transport administration.
- Sis (2015). Teknisk specifikation SIS-TS 39:2015 – Mikrobiologisk renhet i operationsrum – Förebyggande av luftburen smitta – Vägledning och grundläggande krav. Sis Förlag AB 2015 ↩︎
- Lidwell OM et al. Effect of ultraclean air in operation rooms on deep sepsis in the joint after total hip or knee replacement – A randomized study. Br Med J 1982; 285: 10-14. ↩︎
- Global Surg Collaborative. Surgical site infection after gastrointestinal surgery in high-income, middle-income, and low-income countries: a prospective, international, multicentre cohort study. Lancet Infect Dis 2018; 18: 516 – 525. ↩︎